WHO I AM

Some information about me to begin
My name is Elena Vittoria Longhi, Im psychologist, sexologist with more than 20 year of experience on male and female sexual dysfunction.
I’ve been working in the Urology Department at San Raffaele Scientific Institute in Milan, Italy, (Head physician, Prof. F. Montorsi) and I’m dealing with psychologic and sexologic support to urologic and andrologic patients.
Previously I worked in the Urology Department at Humanitas Scientific Institute in Milan, Italy (Head physician, Prof. G. Guazzoni).
My main skills are the psychologic support to oncologic patients in their whole treatment process, as well as the treatment of any sexologic correlate issue especially after radical prostatectomy and cystectomy. Neuro-sexologic approach to urologic, oncologic and andrologic patient is my main interest.
In my free time I play sport, especially open water swimming and gym. When will I practical diving.
I often go to the cinema and theatre, I'm interested in art up to the early ' 900
I have a two year old maltese dog named (King) Arthur. I like traveling and walking in the mountains, especially in the summer, over 2000 meters.
In addition to the professional scientific readings, i like novels that deal with family histories
-

My work at the hospital
I take care of cancer patients from the time of the histological, then in postoperative hospital stay and
-

My husband
Travel is a family passion. My husband is a pharmaceuticals engineer
-

My passion competition
I was European champion and Italian from 7 to 15 years. Then the study took all my time
-

ARTHUR (KING)
Gentle, playful and affectionate. With us for two years at home and on the go
-

Arthur loves homemade grooming
-

Puppy at 2 months
MY EXPERIENCES

Neuro-psychiatric Rehabilitation
1994-1995 Dragonato Psychiatric Center , Bellinzona (tutor drssa C.Meier), CH –
1992-1993 San Paolo Hospital,Pediatric and Neonatology Dep, Milan, Italy, dyrected L. Giovannini.DhPr . Pediatric and neurological disorder: the family relationship
1994-1996 Psychiatric Center, Lugano (dyrected Daguet Prof.), CH - Psychiatric and neurological disordors in patiens with diagnosis of paranoid sindrome, schizophrenia, alcoholism.
1993-1994 Psychiatric Unit USSL 71 Valenza (Al), Alessandria, Italy, dyrected Massimo Pietrasanta Prof : family therapy in psychiatric, behavioral disorders, schizoid and impact on family. – SERT : Unity Addiction and family therapy. Substance abuse behavioral disorders, neurological , sexological and relational rehabilitation. Relational impact on the couple and the family of behavioural disorders in the outbuildings, with brain injuries.
1995 Polytechnic University of Turin, Department of biomechanics. Prosthesic rehabilitation after surgery, procedures and techniques neurosessuologico. Penile prosthetic surgery, neuro-rehabilitation after orthopaedic sexological and behavioral disorders.
2008-2009 Sexual-Surgery Cardiology Director at the hospital, cardiac surgery and Cardiology Department Towers of Ancona, Ancona (Gian Piero Perna Chief), sponsored by the Italian Association for the advancement of Cardiology and the cardiac surgery O.N.L.U.S. Sez. Brands. T
EDUCATIONAL VISITS

LECTURES
1994-1997 Teacher at the "Centro Milanese di Terapia della Famiglia", a partnership with the University of Milan–directed by Prof. Luigi Boscolo and Gianfranco Cecchin. Teacher in the 3rd and 4th year of residency in the hospital and in rehabilitation after surgery clinic. Neurological rehabilitation in the context of the systemic approach and relational-emotional impact on the family
Since 2000 Teacher at the International Institute for Sexology (Chairman Prof. w. Pasini) in Florence in Clinical Sexology oncological, neurological, psychiatric issues applied, clinical and cardiological hospital. Neurological rehabilitation and sexuality in patients with neurological lesions, spinal cord injury. Fix sexual and neurological development of adolescents and adults with autism, Williams syndrome.
Since 2000 the Chair of Urology IRCC San RAFFAELE, University Life and health. Milan with six-monthly educational seminars on interview techniques Andro-sexological treatment and rehabilitation Uro-Oncology neuro-Urologic Surgery Sexology
Since 2006 the session SEXOLOGY COORDINATOR SIA (Italian society of Sexology) with research protocols, teaching for Postgraduates in various Italian locations.
Since 2016 adjunct professor in Clinical Sexology at Chair of Urology and Andrology, University of medicine and pharmacy, Master in Trieste
Rectocele surgery is applied to women between 40 and 60 years. Correction of rectocele repair biological prostheses with transperineal biopsy seems the best practice, since it can reduce some complications associated with the use of synthetic grafts. However often overlooked the body awareness of these women as the difficulty filming a sex life. The partners sometimes are unprepared and tend to protect the partner, to evade the intimacy. Even under these conditions the sexologist, presented as a facilitator of the healing process, it may significantly help surgeons and patients. www.elonghi.it
POSTOPERATIVE oncological and REHABILITATIVE activities

Rehabilitative activities
1994-1996 Santa Maria Goretti Oncological Hospital, Latina, Italy,Department of medical oncology , dyrected M. d'Aprile Prof.
1994-1995 Melzo Central Hospital, Department of Gynecology and obstetrics, Terri b. Ferrante, chief resident. Free Professional advice in rehabilitation counseling in surgical oncology, sexological in female sexual dysfunction and menopausal disorders.
1996-1997 University Vita & Salute, San Raffaele hospital, Department of Clinical Oncology, Rome, directed by Cora Sternberg Chief.
Since 1997 Pius XI clinic in Rome, Urological Laparoscopic and ROBOTIC Surgery Center, directed by Vito Pansadoro Chief: neuro-urological and sexological Rehabilitation afhter surgery
1994-1995 University Federico II, Department of urology and nephrology surgery Endourological stone therapy, Naples. Freelance report in collaboration with D'Armiento and Iacono Chief. Neuro-rehabilitation research protocols, setting uro-sexological to patients with prostate, kidney, bladder ca. Preparation and postoperative counseling in patients undergoing dialysis and organ transplantation.
1998-2001 Rome American Hospital, Department of Urology, Oncology and Senology, headed by dr Antony Fiore and dr Charles Calvi Chief. Rehabilitation after surgery and breast ca/sexological psychoncological in lung, prostate, bladder ca ca. Neurological rehabilitation in PCs with brain injuries and spinal cord to brain injury. Clinic for medium to severe neurological and psychiatric syndromes
Dal 2000 Sexual Medicine Center, Università Vita Salute San Raffaele, Milan, conducted by Professor Urology Unit, Patrizio Rigatti Chief and Francesco Montorsi, scientific director . Professional relationship in Clinical Sexology of male and female sexual dysfunction, fertility treatment, supportive care postoperative rehabilitation urosessuologica at the Division of metabolism disorders, conducted by Renzo Colombo Chief.
2002-2004 Bolzano Central Hospital, Department of Urology, Armin Pycha Chief. Rehabilitation service for patients with bladder and prostate cancer.
Since 2010 University Hospital of Bologna, Policlinico s. Orsola-Malpighi, Andrology Dep. directed by Fulvio Colombo Chief.
SURGERY AND SEXUALITY

Surgery and Sexuality?
Is the marriage of Robotic surgery and sexology possible?
What does this haveto dowith the surgeon? Two pilot studies from Memorial-Sloan-Kettering cancer Center, examining psychological distress in men with prostate cancer and their partners, suggested that the partner plays an integral role in the patient's adjustment totreatment. (Copeland GP, Jones D., Walters M.Possum, Ascoringsystem forsurgical audit.Br J. Surg 1991; 78:355-360)
My study : Two homogeneous groups of 120 patients were montly administred (15 days afther surgery and for abaut one Year) some invalidated instruments: FS36-EDITS,IIEF,IPSS, SSLR,EES,MAT-R + Pharmachoterapy for ED and sexological counseling. Fullow up
The results : SEXUAL ACTIVITY was spontaneously recovered by 10% monolateral Nerve sparing and 56% bilateral nerve sparing. ERECTILE FUNCTION 59% submitted to pharmachoterapy.
Partners Therapeutic Control: 87% of partners collaborated afther Robotic Surgery. Depression level (90-120 days afhter surgery) 48% of the patients Loss of self-esteem in patients withe sexual problem prior the surgery: 51%. Couple conflict in patients with urological and sexological problems: 23% Patner's depression afther surgery: 38% Loss of male body identity: 34%. Patient's partner desertion: 1%.
Robotic surgery provides the Protocol of my study: taking charge, 15 days after surgery, the onset of pelvic floor rehabilitation, Surgery and rehabilitation sexological's visit.
The sexologist not only erectile rework and sexuality with your partner. Shares with the patient and partner neurovegetative changes in stress afther surgery.
-

FEMALE SEXUAL DYSFUNCTION
The relationship with the body, pleasure, sexuality and the opposite sex ... often at the base of female sexual discomfort
-
MALE SEXUAL DYSFANCTION
The relationship with femininity, emotional liability, fear of abandonment, sexual failure. ...
-

SEXUALITY AND....
Surgery (varicocele, circumcision), recurrent bacterial prostatitis, erectile dysfunction, diabetes and multiple sclerosis and ...

Prostatic hypertrophy and absence of Cumming. A handicap male often poorly investigated but that oppresses men's sensitivity, reduce sexual role, creates inadequacy in a relationship
Implantation of penile prosthesis is a surgical location and relationship. Prepare the patient to the plant, follow him during the hospital stay and train the new sexuality is a "custom" process. Different the premise of a diabetic patient, a prostatectomizzato or a young in neurological patients. The partner, not always active in these locations are the therapists unaware of a good quality of life and a successful surgery. www.elonghi.it
SEX AND CONDOM
A limit for many men of sensibility, sexual potency, and for her?

It is true that patients lie to your doctor? A recent study by the Department of Psychiatry of Arkansas reports that 59% of the patients mind at their Specialist especially when it comes to obesity or sexual disorders. The 78% does not abandon the specialist even if cures are ineffective, the 4% does not employ the therapies and the 68% hoped that the specialist ask of sexuality ... Why so much reticence? www.elonghi.it.

Many erectile dysfunction in men between 30 and 45 years depend on pornographic video dependency. Passive viewing of footage exciting and gradually increasing the perception of pleasure, changes over time in the central nervous system. Therefore, in relation to two, the partner has an extremely short excitation time and mostly level exclusively. The partners presented low participation of the other and a too rapid and poorly lasting sexual response. Andrologist more experienced in these cases requires a consultation sexological and hence an empathic therapeutic contract and high achievement. www.elonghi.it
THE COMMUNICATION WITH THE PATIENT

Communication with the patient is an art, a style that depends on the personality of the physician and affecting more than 60% of therapeutic compliance. A severe diagnosis can be shared with empathy, participation and scientific knowledge. Emotional intelligence: know = Clinic: therapeutic style. Being able to communicate is a tool to speed up treatment, to simplify the relationship with the patient and family members, as well as add value to scientific knowledge. www.elonghi.it
PATIENT AND PARTNER WITH ORGASMIC DISORDER?

How to approach a patient with Orgasmic disorder with a female companion pretending the pleasure? Faking orgasm is still widespread among women, often aimed at avoiding the pleasure. It seems strange but there are people, men and women, who are afraid to be happy. Many disorders of the male and the female orgasm Cumming depend on a phobia to each inner concealed enjoyable not attained by suffering and effort. The male and female body image is as if trying to hide the taste of transgression. Consult a sex therapist can be a way to resume a "new contract" with one's own body and the sexual role. www.elonghi.it
Genital psoriasis and sexuality. Many young men complain of burning, itching, flaking genital areas. The partners often demand more frequent intercourse, greater initiative and passion. The partners describe an autoerotic activity almost daily, an eroticism fantasized and little lived, pornographic video dependency and a suffering in solitude ... www.elonghi.it
Surgery, chemotherapy, radiotherapy: many women diagnosed with breast cancer, are familiar with this process. The pastor are very attentive to the reactions of women in clinical treatments, the emotion, the emotional feedback. The sexologist instead turns them "tomorrow's bread", to reflect on the changes of the body, relationships and body awareness. Sex talk can sometimes seem out of place, but the intimacy of a woman refers, in addition to the relationship with the partner, their own seduction. By your own way of being a woman ... always! www.elonghi.it
COLORECTAL CANCER AND SEXUALITY
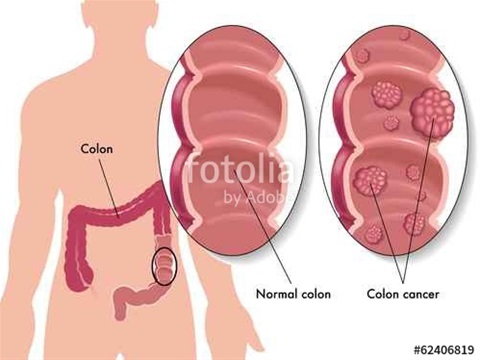
Colorectal Cancer: often affects young patients with a quality of life that need reviewing and reinvent. Surgeons of this discipline may offer, with much tact, that life doesn't end with the newfound health. The cost for new life may not require sacrifices and limitations. In these cases the sex therapist does not concern only the resumption of intimacy, but it reflects on the changes the patient's sensitivity, body scheme, on the fear of the resumption of the disease, a second man. With a body to recognize and improve. www.elonghi.it
What happens when a patient has a partner with endometriosis? Endometriosis is a condition suffered by many young women. Hard to live a sexuality complacent and find harmony your body. Gynecologists should recommend a consultation sexological, besides medical therapy. Every patient has the right to review their own body image and return to a more suitable relationship to herself a femininity complacent and complicit. www.elonghi.it
THE ROLE OF THE SEXOLOGIST IN UROLOGY

The Urologist (Andrologist) and Sexologist
INTRODUCTION AND OBJECTIVES - The objective of this study was to evaluate the cooperation with sexologist in daily andrological practice in order to prevent somatization of psychosexual problems and to improve patient compliance.
MATERIALS & METHODS – 116 heterosexual married couples between the ages of 30 and 48 were recuited (in a stable marriage for 3 to 15 years). 58 patients had to have been suffering from PE for at least 2 years and 58 patients had to have been suffering from DE for at least 2 years . The following questionnaires were administered in this order: International Index of Erectile Dysfunction (IIEF), the Hamilton Depression Evaluation Scale (HAM-D). Each partner was administered the following: Female Sexual Function Index (FSFI), Brief Male Sexual Inventory (BMSI), Measuring Marital Satisfaction (MMS-3G), Sexual Satisfaction Scale (SSS), The Conflict Tastics Scales (CTS). Afterwards there was an individual check up interview (also using the Operationalizing Premature Ejaculation, G.Grenier et al., University of New Brunswick, 1997, Canada) and one as a couple.
RESULTS – The large proportion of female (35%) and male (10-25%) andrological patients had traumatic sexual experiences in the past; 18% patients with negative and traumatic experiences with urogenital medicine, and 23% patients with urological, sexological and/or psychiatric comorbity. Also, 8% patients with sexual and gastrointestinal comlaints.
CONCLUSIONS – In the evaluation of a sexual dysfunction it is necessary to realize that irrespective of the cause of the (erectile and ejaculatory) disfunction there always will be secondary psychological reactions that may aggravate the sexual dysfunction and/or influence coping, sexual relationships and therapeutic comliance.
LAPAROSCOPIC PROSTATECTOMY AND SEXUAL REHABILITATION
INTRODUCTION – The study assessed 360 nerve sparing Radical Laparoscopic Prostatectomies followed by neurosexological rehabilitation and traditional pharmacoterapy.
MATERIAL AND METOD – Patients, recruited in three years, were monthly presented (15 days afther surgery and for about one year) some self administred validated questionnaires:SF 36,EDITS, IIEF, IPSS, SSLR, EES, CES-D, MAT-R. There followed, during the post surgical sexual rehabilitative phase. Two individual interviews with the patient, an individual interview with the sexual partner, 2-3 interviews with the couple. Pharmacoterapy for ED, following Montorsi’s protocol, was associated to neurosexological rehabilitation from second week afther surgery. Pharmacotherapy is combined with sexual rehabilitation’s exercises. Follow up: monthly during the first year, every three months during the second year. Every six months during the third year.
RESULTS – Sexual activity was spontaneously recovered by 6% of monolateral nerve sparing patients; with the pharmacotherapy 56% of patients had erectile recovery. In bilateral nerve sparing: spontaneously recovered by 28%, that must be added to 30% of recoveries using pharmacoterapy. 78% female partners collaborated in the sexual rehabilitation. There was an additional 18% of occasional partners sexuality. Every femal partner had a terapeutic role in the relationship/seeking of a new sexuality.
CONCLUSIONS – Sexological rehabilitation has revealed a synergic and essential multidiscilinary approch in sexual activiy recovery even cases of partners opposition to the administration of pharmacoterapy for ED.
PREMATURE EJACULATION (PE) AND INFANTILE NOCTURNAL ENURESIS

ENURESIS and PREMATURE EJACULATION
INTRODUCTION AND OBJECTIVES – We studied the correlation between Premature Ejaculation and Infantile Nocturnal Enuresis in 75 subjects, affected by non physiological PE from the first instance of sexual intercourse.
MATERIALS AND METHODS – The subjects, average age 38 with a partner of at least one jear’s standing, were administered the following: DSI-R “Differentiation of Self Inventory”, SRO “Sex-Role Orientation Scale”, IMS “Index of Marital Satisfaction”, ISS “Index of Sexual Satisfaction”, HAM-D “The Hamilton Depression Evaluetion Scale”, AMS “The Aging Male’s Symptoms Scale”.The subjects complained of secondary enuresis at schoolage with episodes varjing from 2-3 times per week for at least 1-2 years. The first sexual intercourse ith the appearance of PE occurring between 17 and 25 years of age.
RESULTS – The data revealed that 47% of subjects had difficulty sleeping, suffered from irritability and excessive perspiration combined with a general decline in physical ability and beard growth. 63% showed a decrease in spontaneous morning erections. An excessive dependence on the partner was exhibited by 32% while 21% earned less than the partner. 19% found sex a chore, 15% experienced difficulty making decisions in the absence of the partner, 37% were unable to feel pleasing for the partner while, 12% were inclined to do everything in a rush and 9% found it difficult to accept pleasure.
CONCLUSIONS – The study seems to show that PE, in particularly emotional and insecure subjects, substitutes, in adult age, infantile nocturnal enuresis. It demonstrates the difficulty the subject has in controlling emotions and dealing with the beat of the female world.
UNCONSUMED MARRIAGES AND SEXUALITY

Unconsumed Marriages
INTRODUCTION & OBJECTIVES: The present study investigated the aspects of the relationship and sexuality of couples in unconsummated marriages using validated questionnaires and specific counselling in order to allow partners to discover an intimacy in keeping with the communicative style of the two.
MATERIALS & METHODS: 32 couples between the ages of 28 and 40 were (average age 34) were recruited, having been married for at least seven years and having known each other or been engaged beforehand for one to two years. Each partner was administered the following: Measuring Marital Satisfaction (MMS-3G), The Conflict Tactics Scales (CTS), Sexual Satisfaction Scale (SSS), Communication Patterns Questionnaire (CPQ), Questionnaire for Reproductive Emotionality (QER). Afterwards there was and individual check-up interview and one as a couple. While the sexological counselling for couples finished on average after 5-8 fortnightly meetings the follow-up at the and of counselling was carried out at 6 months and 1 year.
RESULTS: The couples were homogenous never having had sexual experiences other than with the partner. The trend is to exclude open verbal conflicts for fear of being abandoned or of assertion (more often than not physical) by the other partner. They exclude passionate erotic impulses and sensations as they are associated with violent acts. Sexual teachings and the creative aspects of sexual games is entrusted to one partner. Disagreement on times and ways of spending time together is also due to the timing and ways intimacy is desired, sought and experienced. Mainly romantic and affectionate in the couple and erotically transgressive in autoeroticism. Both partners pursue fantasies and desires of betrayal without follow up. Very often the desire for the child pushes the couple to face the sexual problem but not always to live intimacy in and of itself.
CONCLUSIONS: The sexological counselling to bring to life unconsummated marriages foresees a psycho-educational space were each partner is free to ask for information and redefine prejudices an fears on sexuality. The individual sexological exercise and those performed in couples, together with interviews as a couple have been a valid support in redefining in the couple emotive needs and sexual timing as well as expressing fantasies and desires. 11 couples out of 32 have had a child.Sono un paragrafo. Clicca qui per aggiungere o modificare un testo. Qui puoi raccontare ai tuoi visitatori chi sei e qual’è la tua storia.
A PSYCOSEXUAL STUDY OF SEXUAL FUNCTIONS DURING PREGNANCY

FAMILY AND SEXUALITY
INTRODUCTION AND OBJECTIVES - The objective of this study was to evaluate the sexual functions during pregnancy and to retrace the emotive, relational aspects with the help of questionnaires validated at international level, psycosexual counselling and a ginecological-urological examination.
MATERIALS & METHODS – 55 women (26 in the second and 29 in the third trimesters of pregnancy within a stable relationship) between the ages of 26 and 40 were chosen in this study with their partner. Each partner was administered the following: Female Sexual Function Index (FSFI), Measuring Marital Satisfaction (MMS-3G), Questionnaire for Reproductive Emotionality (QER), Communication Patterns Questionnaire (CPQ). Afterwards there was an individual check up interview and one as a couple. The scores between the first, second, and third trimesters of pregnancy was performed using Wilcoxon’s signed-rank test: differences considered at P<>
RESULTS – The frequency of intercourse attempts during the last 4 weeks was 9.6 +/- 4 before pregnancy, and 5.9 +/- 3.5, 4.6+/-3.6, 2.1+/- 1.8 in first, second, and third trimesters of pregnancy, respectively. With regard to FSFI, except for desire, arousal, lubrification and orgasm (sexual dysfunction are related to hormonal situations), were not significantly different between the first, second, third trimesters of pregnancy.
CONCLUSIONS – The frequency of intercourse attempts was significantly decreased with the increasing gestional age. Childbearing couples, the partner particularly, asked for information abaut sexual problems and fluctuations in patterns of sexuality during the pregnancy.
PREMATURE EJACULATION IN HETEROSEXUAL COUPLES

INTRODUCTION AND OBJECTIVES - The present study investigated the efects of the relationship and sexuality of couples of the impact of premature ejaculation (PE) functioning. Using validated questionnaires and specific counselling in order to allow partners to voice their feelings.
MATERIALS & METHODS – 98 heterosexual married couples between the ages of 28 and 48 were recuited (in a stable marriage for 5 to 15 years). The patients had to have been suffering from PE for at least 3 years. Each partner was administered the following: Female Sexual Function Index (FSFI), Brief Male Sexual Inventory (BMSI), Measuring Marital Satisfaction (MMS-3G), Sexual Satisfaction Scale (SSS), The Conflict Tastics Scales (CTS). Afterwards there was an individual check up interview (also using the Operationalizing Premature Ejaculation, G.Grenier et al., University of New Brunswick, 1997, Canada) and one as a couple.
RESULTS – Duration of marriage was not a significant factor in the results. 76% of female partners’ estimates of ejaculatory latency were shorter than were the men’s estimates. Usually, the women perceived their male partners to ejaculate too quickly less often than was reported by the men. 65% men with PE reported lower pleasure and enjoyment associated with orgasm and 34% described differences in relationship satisfaction and 78% in the requency of intercourse. 53% reported that effective appraisals of their PE status affects their sexual functioning more generally. 13% men with PE reported DE for 1 to 2 years also.
CONCLUSIONS –PE has a negative impact on the sexual satisfaction of heterosexual couples. PE is associated with having more other non PE sexual concerns for men, but not for their female partners.
Recurrent prostatitis and sexuality
INTRODUCTION AND OBJECTIVES - The purpose of this study was to track the emotional causes, neurovegetative and sexual relations, the ED young-adults with recurrent prostatitis patients for at least a year.
MATERIALS AND METHODS -Were recruited 100 patients aged between 25 and 35 years old, with at least 6 months and a fixed partner ED sex from three to six months, with a history of recurrent bacterial prostatitis surgery clinic. Were administered in the following order: International Index of Erectile Dysfunction (IIEF) Evaluation, the Hamilton Depression Scale (HAM-D). Each partner was administered the following: Female Sexual Function Index (FSFI), Brief Male Sexual Inventory (BMSI), Measuring Marital Satisfaction (MMS-3 g), Sexual Satisfaction Scale (SSS), The Conflict Tastics Scales (CTS). These were followed by an interview of control and three psicosesuologici talks. Clinically, each patient had been prescribed an antibiotic therapy repeated over time and an oral therapy for erectile dysfunction in low dosage one day.
RESULTS. These anxious-depressive traits: HAM-D 26.8 +/-1.80 and Italian version of the CES-D 29.4 +/-1.5. In terms of self-esteem (Italian version of the RSES) is greater than the feeling of inadequacy and indefiniteness of body image (37.6 +/-8.2), alta (DSI-R) depending upon the expectations of partners (56.2 +/-1.4), as well as the rivalry towards her (34.3 +/-1.1). The IIEF showed an incidence of 64.1 ± 2.4 none of the patients took oral therapy for DE prescribed even if you bought: symptom remission has been declared between the second and third psicosessuologico counseling interview.
CONCLUSIONS. The ED young adult suffering from psychogenic relapsing bacterial prostatitis appears mixed anxiety-depressive syndrome, caused by high stress competitive roles at work and in the conduct of psychogenic in sexuality, low threshold of frustration In DE seems emerge even a manly role challenge reached by the patient is to support both the medical team Andrologist (sexologist) as opposed to the relationship with partner often competitive and strong personality